BACKGROUND
In 1886, the Benedictine Sisters of Italy and the Presentation Sisters of Ireland came to the Dakota Territory to start schools. Their faith eventually led them to build hospitals to support diphtheria and influenza epidemics. Though the 2 groups had slightly different beliefs and few resources, they remained steadfast in their dedication to their ministry to care for the sick. They managed to construct many hospitals over decades to serve multiple small regions, but eventually the sisters decided to combine their efforts and cosponsor a unified health care system. They knew this collaborative effort would strengthen their ability to serve the people of their region. Thus, the organization known today as “Avera,” meaning, “to be well,” was born.1
Fast forward to 2024: Avera’s integrated health system with over 300 health care facilities spans over 72,000 square miles, 5 states, and 86 counties.2 Sioux Falls, South Dakota, is the system’s primary point-of-care, with specialty physicians, pharmacies, and nurses able to meet the needs of patients with complex conditions that require specialty medications and ways to administer these treatments. Home intravenous infusion therapy has become more popular due to many factors. The 2 major components driving an increase in demand are cost-savings associated with home infusion in comparison to the hospital outpatient setting and site-of-care restrictions imposed by payor sources.3 Avera Home Infusion Pharmacy (AHI) followed in the footsteps of its founders to meet this challenge by admitting their first specialty infusion patient on November 16, 2018. Currently, AHI provides services for 173 specialty infusion patients. This small, yet innovative pharmacy has developed a multidisciplinary approach that allows for standardization of processes, improvement of patient outcomes, and provision of cost-effective, quality care to its patients. As AHI continues to expand, the focus will continue to be to provide specialty infusions to its rural locations, just as the Sisters did with their hospitals long ago.
Since 2019, one of the fastest growing areas in home infusion agencies has been specialty infusion.4 There are many barriers to overcome in providing specialty infusions to patients in rural and remote locations, which include congested outpatient infusion centers, site-of-care restrictions, costs, and other logistics. Due to the increased volume of patients needing specialty infusions, outpatient infusion centers have limited chair availability. Higher overhead drug pricing has also caused many commercial payors to impose site-of-care restrictions, which forces patients to either utilize home infusion or face out-of-pocket costs for their outpatient infusions.3 As a result, the availability of home infusion in most rural areas is limited or non-existent. Between 2005 and 2018, home health grew nearly 37%.5 Home infusion care facilities in rural areas are experiencing shortages in trained nurses and pharmacists who are essential for administering and overseeing specialty infusions. Specialty infusions require specific nursing knowledge and expertise to be safely administered in the home. Patients in rural areas face additional financial challenges in accessing specialty infusion centers due to long travel times, vehicle procurement and dependability, travel and hotel expense, and severe weather conditions. Specialty infusion drugs cost an average of thousands of dollars per dose and are further complicated by insurance authorization processes, denials, and patient access to drug assistance programs.4 Pharmaceutical manufacturers provide copay cards, which help patients cover their high deductible and out-of-pocket costs.6 Talented and engaged billing representatives are crucial to navigating insurance and copay programs to ensure drug coverage.
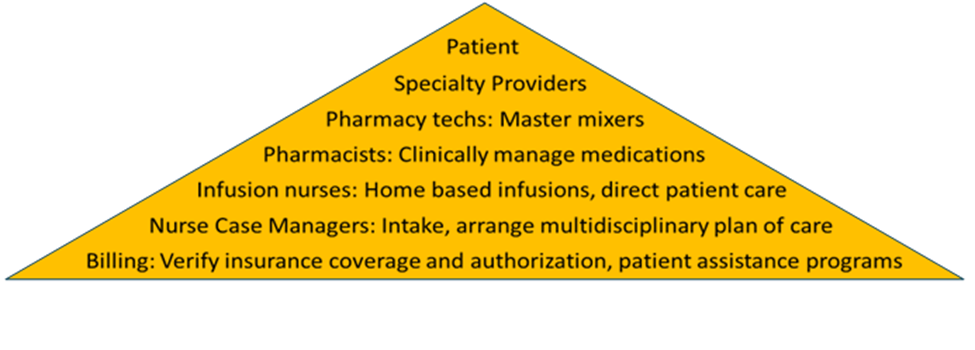
Avera Home Infusion Pharmacy has created a highly skilled team to assist patients transitioning to home infusion. The staff includes 5 Pharmacy Technicians, 4 Pharmacists, 1 Patient Advocate, 1 per-diem and 3 full-time registered nurses (RN) Case Managers, 1 full-time Specialty Infusion Nurse, and 2 intake Insurance Specialists, all of whom are overseen by the Pharmacy Director (Figure 1). Each role plays a significant part in achieving AHI’s goals. Some of the Pharmacy Technicians’ duties include compounding pharmaceuticals, packaging supplies needed for infusions, and ordering all the inventory required to operate the pharmacy. Pharmacists oversee the Pharmacy Technicians and clinically manage medications by contacting patients periodically to coordinate shipments of medications and supplies and by monitoring routine lab work to ensure therapies are not contraindicated by acute health issues. The Patient Advocate is a Pharmacy Technician, who acts as a liaison between patients and various copay assistance programs by enrolling the patients in appropriate programs and submitting bills to the copay cards to decrease drug costs. The RN Case Managers are responsible for screening initial referrals to ensure the patients have appropriate payor sources and that they have access to home care services or outpatient centers in their areas. The Specialty Infusion Nurse provides direct patient care in patients’ homes by administering specialty infusions, monitoring for adverse reactions, and contacting providers for current orders. Insurance Specialists verify patients’ benefits coverage and obtain prior authorizations for medications. Though their roles are specialized, all members of AHI work together as a team to ensure optimal patient care and cost efficiency. Figure 2 shows current home infusion patient census by therapy type.
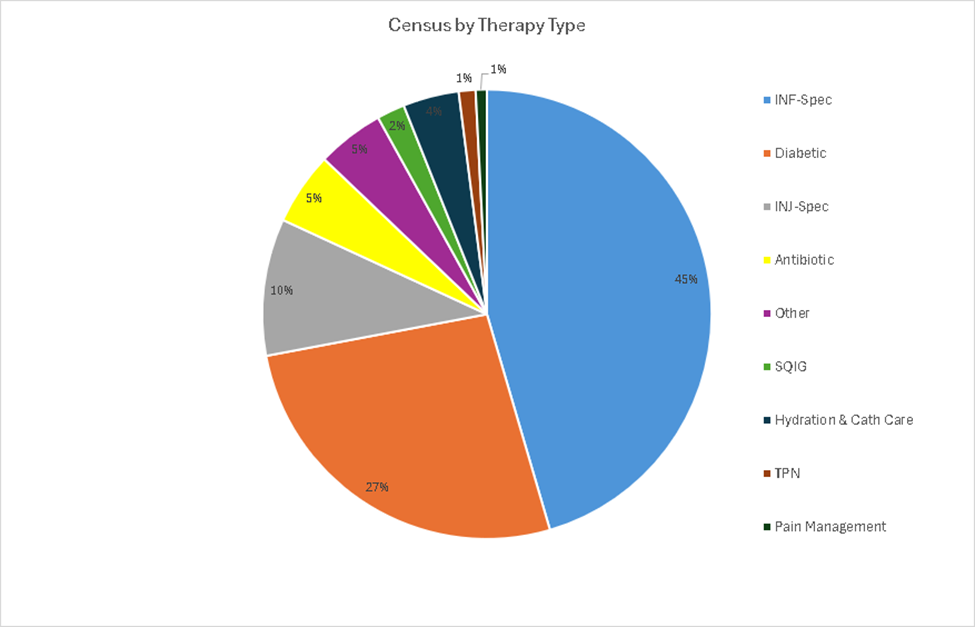
Abbreviations: cath, catheter; INF-Spec, infusion-specialty; INJ-Spec, injection-specialty; SQIG, subcutaneous immunoglobulin; TPN, total parenteral nutrition.
CASE STUDY
Patient A is a 61-year-old female diagnosed with Ulcerative Colitis in 2014. Her medical history also includes chronic obstructive pulmonary disease (COPD), hip and knee replacements, chronic pain, and morbid obesity with a body mass index (BMI) of 62.4. She works full-time and lives 60 miles from the nearest outpatient infusion center. She receives Infliximab IV every 8 weeks. Her total infusion time in the infusion center is 3 hours with additional drive time of 2 hours. In the winter months, her trip can take up to 4 hours. Due to the patient’s chronic pain, her spouse needs to take a day off work to transport her to and from the infusion center. The patient was relieved and excited when she found out her insurance wanted her to do her IV infusions at home. The biggest challenge for Avera Home Infusion Pharmacy was to find a home health nurse to administer her infusions. The home care in her area was already overwhelmed with other patients and was unsure that they could accommodate a specialty infusion. To solve this problem, AHI collaborated with the peripherally inserted central catheter (PICC) nurse at a rural hospital in Pierre, SD. The PICC nurse learned to provide education to the IV antibiotic patients who were consuming a lot of resources for the home care agency. Teaching these patients at the hospital now meant the home care nurse did not have to go through the lengthy admission process for new IV antibiotic patients. These patients could now have their weekly PICC line dressing changes and lab draws at the outpatient infusion center. This partnership allowed the home health care nurses in Pierre the time to train and perform specialty infusions in their rural area. This allowed Patient A to remain in the comfort of her home to receive her 2-hour infusion. Avera Home Infusion Pharmacy’s Patient Advocate team also enrolled her in a drug assistance program to help with her medication’s overall cost. Her spouse is also free to go to work and does not have to take time off to transport her to her infusions. The AHI pharmacy innovatively collaborated internally and externally to ensure access to home infusion not only for Patient A, but also for many other patients in rural areas of the Avera system footprint.
The project aims of AHI are to increase the volume of specialty infusion patients it services, to increase the number of home health care agencies administering specialty infusions in patients’ homes, and to provide cost savings to patients by enabling them to utilize home infusion instead of outpatient infusion centers, all while maintaining a high patient satisfaction rating with home infusion services.
METHODS
The first test solution developed to achieve the aims of AHI was creating more availability for Avera home health care nurses by diverting patients from home care to other resources within the community when able. When patients in need of long-term intravenous antibiotic therapies were previously discharged from the hospital, AHI Case Managers arranged for their initial teaching, labs, and IV catheter care to be performed by home health care nurses in the patients’ homes. This caused the home care agencies to be too saturated and, therefore, unable to dedicate the staff to learn or administer home infusions. To change this circumstance when needed, AHI Case Managers triaged patients either to themselves, or to outpatient infusion centers local to patients’ residences instead of home care agencies. For instance, when the patient was discharged from Avera’s largest hub hospital in Sioux Falls, Avera McKennan, an AHI Case Manager performed the patient’s initial teaching. Then the nurse partnered with an outpatient infusion center in the patient’s local area to schedule weekly labs and dressing changes rather than relying on a home care agency. This would allow a home care nurse to be available for a specialty infusion instead, if needed. Additionally, if a patient was discharging from a rural community hospital within the region, the Case Manager collaborated with that hospital’s outpatient infusion center to complete the patient’s initial teaching, weekly labs, and dressing changes at the patient’s local hospital. Utilizing these other resources, particularly in underserved, rural areas allowed home health care agencies the availability to learn and perform longer specialty infusions, which made home infusion available for patients who otherwise would not have this option.
The second test solution developed to achieve AHI’s aims was providing adequate specialty infusion training and support for home health care agencies within the Avera region. Home health care agencies in rural communities within the Avera Home Infusion footprint had limited knowledge and training materials available to their staff prior to this intervention. Furthermore, many of the agencies only encountered the need to service specialty infusions on rare occasions. The tasks of learning and administering infusions on their own were daunting to them. Initial discussions with each home care agency opened doors for change and improvement of home infusion practices. Subsequently, AHI’s Case Managers created an ongoing monthly liaison group meeting with Avera Home health nurses and leaders to discuss and provide education based on each agency’s questions and concerns regarding specialty infusions. Pertinent education topics are chosen and formatted into a monthly newsletter, providing an efficient, evidence-based, and consistent method to educate all staff within each regional agency. To further support each home care nurse and patient, detailed specialty infusion education sheets with step-by-step administration instructions specific to each patient’s needs are sent to the home with supplies and medications. These processes create a feedback loop for resources and resolving issues to support the home care nurses.
Throughout these 6-year partnerships, AHI has gained the trust of home health agencies across its region and has provided them with adequate education to feel comfortable and competent to administer home infusions. Avera Home Infusion Pharmacy also provides home care agencies with contact numbers of pharmacists and nurses who can provide immediate assistance to nurses in patients’ homes to troubleshoot issues and address any questions promptly. In turn, AHI gained the ability to refer to several home care agencies in its region, many of which were previously unavailable for the tasks of specialty infusions.
The third test solution was to provide a safe and cost-effective option for specialty infusion patients in their homes. AHI has insurance intake specialists completing insurance prior authorizations and appeals for specialty infusion. This is to ensure patients receive the correct drugs and that their drugs are in network with their insurance providers. Having dedicated subject-matter experts helps the pharmacy to work efficiently and ensure the correct documentation is submitted for prior authorizations with insurance companies, expediting patient care. Avera Home Infusion Pharmacy also has Patient Advocates to assist and ensure each patient is enrolled in a copay drug assistance program. This not only covers the cost of the medication, but also, at times, can cover the home health care nursing services when patients’ annual deductibles have not yet been met. The Patient Advocates also submit bills to the copay drug assistance cards for the patients once each infusion has been completed. This process has allowed AHI to pass these cost savings on to its specialty infusion patients.
MEASUREMENTS
Three measurements were taken to track the success of implementing the solutions. First, AHI obtained monthly data on specialty infusions performed by home care agencies, which were categorized by each individual agency. Second, surveys were simultaneously sent out to the Home Health nurses to evaluate staff members’ comfort in administering specialty infusions. The third measure tracked the amount of money billed to drug assistance copay cards over the past 3 years, which represents overall cost savings to the patient. Descriptive statistics were used to analyze each of the 3 measures.
RESULTS
The primary project aim was to increase specialty infusion in rural health care while maintaining patient satisfaction. By utilizing community resources, AHI increased the availability of home health agencies to complete home infusions. Figure 3 shows the AHI specialty patient census, sorted by each home health agency performing the infusion from March 2022 to December 2024. Note the steady incline in the specialty infusion patient census with the current number at 173. Also of note, there was an overall increase in home health agencies completing specialty infusions. In 2022, there were only 4 home health agencies capable of administering specialty infusions. Table 1 is a snapshot of the current patient census and the home care agencies completing specialty infusions. Currently, 12 agencies in the Avera region are administering specialty infusions. One of the 12 agencies is Avera @ Home in Pierre, South Dakota, which is in a remote area often challenged by staffing issues and winter weather conditions. Avera @ Home in Pierre increased their specialty infusion patients from zero to 10 in just 16 months. This area was in desperate need of home infusion providers, and its patients are now grateful to have these services.
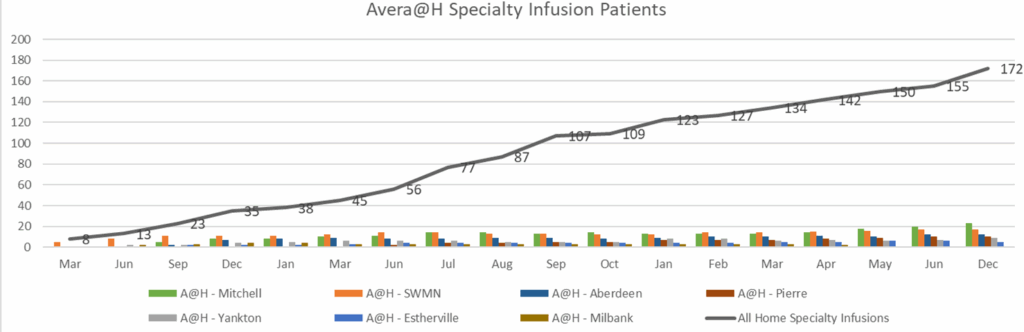
Table 1. Current Home Agencies Performing Specialty Infusions
| Nursing Agency | Number of Patients |
| AHI-Infusion Nurse | 93 |
| A@H – Mitchell | 23 |
| A@H – SWMN | 17 |
| A@H – Aberdeen | 12 |
| A@H – Pierre | 10 |
| A@H – Yankton | 9 |
| Prairie Lakes | 6 |
| A@H – Estherville | 5 |
| A@H – Milbank | 3 |
| Hegg | 2 |
| Redfield Memorial | 1 |
| Sioux Center | 1 |
Abbreviations: A@H, Avera at Home; AHI, Avera Home Infusion Pharmacy.
The secondary project aim was to increase the number of home health care agencies administering specialty infusion at home. This required educating the home health staff and assessing their comfort levels with administration of home infusions. Twenty-two home health nurses completed AHI’s survey. The first survey question was, “How many specialty infusions have you done in the past year?” Responses from the agencies polled were as follows: 13 responded between 0 and 5 infusions, 2 responded between 5 and 10 infusions, 4 responded between 10 and 20 infusions, and 2 responded greater than 20 infusions. The second survey question was, “How comfortable are you with administering specialty infusions?” Responses were as follows: 7 agencies were very comfortable, 10 were somewhat comfortable, and 4 reported they were not comfortable at all. The third survey question was, “How comfortable are you with starting a peripheral IV?” Responses were as follows: 10 agencies responded they were very comfortable, 7 said somewhat comfortable, and 4 said their agencies were not comfortable. Survey question 4 was, “Do you feel comfortable asking questions to AHI staff?” One hundred percent responded “Yes.” These survey results illustrate how many infusions the nurses within the home care agencies have completed and whether they were comfortable in performing the infusion as well as peripheral IV starts. It also demonstrates that AHI was able to build a trusting relationship with its regional home health agencies, of which they can mutually depend upon each other to work together through problems and solutions to ensure patients’ specialty infusion needs are met.
The third project aim was to pass cost savings associated with home infusion on to patients as compared with outpatient infusions. Patients who were previously receiving infusions as an outpatient and transitioning to AHI would often inform intake staff that they had not previously been enrolled in any patient assistance programs. AHI ensures that specialty infusion patients are enrolled in a copay drug assistance card whenever possible. In 2022, AHI invoiced $508,000 to copay savings cards. As impressive as that sounds, AHI saw an increase in specialty infusions and billed over 1 million dollars to copay savings cards in 2023. All the dollars paid by drug assistance cards were applied to patients’ deductibles and annual maximum out-of-pocket amounts that were not met, at times saving them thousands of dollars each.
Within a year of developing and implementing this project, AHI achieved a 79 Net Promoter score (NPS). NPS is a measure of customer experience and predicts business growth. “A Net promoter score of 71 to 100 is considered the holy grail of NPS and is rarely attainable. A company with a score in this range is considered among the best in their industry.”7 AHI can deduce that because home health nurses are feeling more confident in administering specialty infusions, patients have a better experience, which overall leads to superior outcomes.
DISCUSSION
Densely populated areas are utilizing freestanding infusion centers that meet insurance site of care restrictions to reduce costs. In the rural Midwest, freestanding infusion centers do not exist at the present. With great distances between residences and would-be infusion centers, travel times would be long, and likely, the infusion patient population would not support outpatient centers in many areas. By utilizing home infusion and collaborating with home health staff, AHI ensures that patients can get infusions in a cost-effective manner with top-notch care in the comfort of their homes.
LIMITATIONS
The limitations of this study include a large geographic area, vast range of nursing experience, lack of home health staff, and lack of repetition due to infusion infrequency. AHI services 5 states across the rural Midwest, often leading to long travel times from its location in Sioux Falls. The geography of the Avera region did not allow AHI staff to go to each agency to complete in-person training. Avera home health agencies require 3 years minimum nursing experience to become a home health nurse; however, they do not require an infusion therapy background. This can lead to many nurses with vast nursing experience still feeling uncomfortable with administering specialty infusions in patients’ homes. Additionally, rural health care is challenged by employee shortages, including qualified nursing staff. Avera home health nurses across the region also find it difficult to become competent in specialty infusions, given that there is typically a lack of repetition due to infrequency of the need for specialty infusions and the lack of patient population. When AHI staff were able to teach staff in person or go to the first specialty infusion, the transition was smoother, and nursing staff felt more comfortable doing infusions.
CONCLUSION
Avera Home Infusion Pharmacy is comprised of 17 individuals dedicated to optimizing patient care, providing a cost-effective specialty home infusion option, and maintaining high patient and nurse satisfaction for a growing patient population. Creating a team of subject-matter experts within AHI allowed for its innovative utilization of home care and outpatient infusion resources, collaboration to educate and support home care staff, and diligence toward financial stewardship and identifying patient support programs. The organization now has the ability to administer specialty infusions to patients who previously did not have this option by helping them overcome geographical, staffing, financial, and other barriers to receiving specialty infusions at home.
Avera Home Infusion Pharmacy continues to follow the forward-thinking of its founders and mission by taking future steps toward continuing education and support of the Avera Home Health Nurses, as well as by extending resources and education to agencies outside the Avera organization to allow for further expansion of specialty infusions in patients’ homes and availability of resources. This creative model of rural provision of specialty infusions could benefit other specialty pharmacies and health care entities facing similar issues, thereby proactively meeting growing demand for specialty health care services in areas with insufficient resources.
REFERENCES
- Presentation Sisters. Healthcare Ministry | Presentation Sisters. Presentation Sisters. Published October 21, 2020. Accessed January 9, 2025. https://www.presentationsisters.org/ministries/healthcare-ministry/
- Avera McKennan Hospital & University Health Center. Avera.org. Published 2024. Accessed January 9, 2025. https://www.avera.org/locations/profile/avera-mckennan-hospital-university-health-center/
- Haines D. Cost savings: home versus inpatient infusion therapy, a review of the literature. Infus J. 2023;2(3):3-7. doi:10.70776/FSCX6194
- Simpson M, Vermeulen D, Haines D. A multi-center time study of home infusion pharmacist professional services for specialty infusion medications. Infus J. 2024;3(3):5-13.
- Geng F, Mansouri S, Stevenson DG, Grabowski DC. Evolution of the home health care market: the expansion and quality performance of multi-agency chains. Health Serv Res. 2020;55 Suppl 3(Suppl 3):1073-1084. doi:10.1111/1475-6773.13597
- Collins Jr C. The latest developments with copay accumulator programs. Infus J. 2024;30(1):23-26.
- Qualtrics. What Is a Good Net Promoter Score? // Qualtrics. Qualtrics. Published 2024. Accessed January 23, 2024. https://www.qualtrics.com/experience-management/customer/good-net-promoter-score/
Increasing Access to Home Specialty Infusion in Rural Health Care
Nancy Cordell, RN, BSN, Case Manager, Avera McKennan Home Infusion 1020 South Cliff Ave. Sioux Falls, SD 57104 nancy.cordell@avera.org
Tiffany Bergeson RN, BSN, Case Manager, Avera McKennan Home Infusion 1020 South Cliff Ave. Sioux Falls, SD 57104 tiffany.bergeson@avera.org
Kristin Williams RN, BSN, Case Manager, Avera McKennan Home Infusion 1020 South Cliff Ave. Sioux Falls, SD 57104 kristin.williams@avera.org
Nancy Cordell RN, BSN, is currently one of the nurse case managers at Avera McKennan Home Infusion. She received her bachelor’s degree in nursing from Augustana University in May 1990. She began her nursing career in June 1990 at Avera McKennan Hospital as a registered nurse in the oncology unit and worked in the oncology unit as a registered nurse for oncology/hospice, charge nurse, and a nurse mentor for new employees and students until 1999. Ms Cordell also taught clinicals for South Dakota State University (SDSU) 1994-1995. She started working as a home care nurse for Avera McKennan in May 1999. She worked in Home Health as a nurse team leader and triage nurse until August 2002. On August 15, 2002, Ms Cordell began her career as a Nurse case manager for Avera McKennan Home Infusion. She has worked in home infusion for 22 years and has been with the Avera system for 35 years. She has been a member of the Infusion Nurses Society (INS) since 2007 and presented at INS 2024.
Tiffany M. Bergeson, RN, BSN, CM, was born and raised in the rural area of Yankton, South Dakota. Staying close to home, she graduated from Mount Marty University with her BSN in 2015. Her RN career started at Avera McKennan in Sioux Falls, SD on the Neurology stepdown/ICU, which is a main hub for all rural communities. Her clinic experience includes ICU, Home Health, and Home Infusion, all within the Avera footprint. In home health, Ms Bergeson obtained a variety of skill sets, including wound care, disease management and education, specialty infusions, IV antibiotic teaching and line care, etc. While working at Avera Home Infusion, she has been able to formulate and nourish the relationships with providers and patients to increase specialty infusions within their homes.
Kristin Williams, RN, BSN, is currently an RN Case Manager at Avera Home Infusion Pharmacy in Sioux Falls. She received an Associate of Science degree from University of South Dakota in Vermillion in December of 2008 and began her career on the Brain & Spine Unit at Avera McKennan Hospital in February of 2009. She obtained her Bachelor of Science degree in May of 2012 from South Dakota State University in Brookings and transitioned to the role of Case Manager of Avera’s Brain & Spine Unit in 2014, as well as serving as an Adjunct Clinical Instructor for the University of Sioux Falls’s nursing program. In 2019, Ms Williams returned to bedside nursing in Neuro Critical Care. In 2021, she explored clinic nursing at Sioux Falls Specialty Hospital Urgent Care just before pursuing her current role at AHI.
INS contributions
Avera home infusion Case managers collaborated and developed a quality improvement project to increase knowledge about providing specialty infusions in rural areas. Nancy Cordell, Tiffany Bergeson, and Christine Palluck presented this information at INS conference in May of 2024, which gained much interest from the audience, inspiring this manuscript.
Nancy Cordell is the backbone of AHI, having worked as a CM since 2002. She was present at AHI and helped to pioneer the first specialty infusion processes, protocols, and patient admission, which occurred in 2018. Her research of journal articles, rural health care needs, organization history, and rural patient population helps illustrate the challenges that can occur in rural Midwest health care.
Tiffany Bergeson collected pertinent data from AHI and developed it into graphs and charts. She worked closely with home care agencies to develop education for specialty infusions, performed education on site with the agencies, and later implemented the monthly nurse liaison group to serve as an ongoing touchpoint for the home care agencies.
Kristin Williams joined the AHI team post-presentation at INS and helped with writing and editing the existing presentation notes into manuscript form. She also contributed AHI role descriptions and workflows demonstrating the pharmacy’s collaborative efforts, innovations, and teamwork.
All conflicts of interest have been resolved.





